Long Head of Biceps Tenodesis
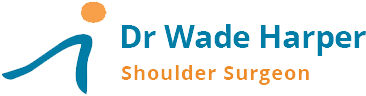
The biceps muscle has 2 attachments at the shoulder (long and short heads) and 1 attachment at the elbow. At the shoulder, the long head of biceps is the more likely tendon to develop problems. The tendon attaches to the top of the socket, runs through the joint and exits into a tunnel that runs down a groove on the humerus, to the muscle. The tendon takes a 90 degrees turn, over the humeral head.


The long head of biceps tendon can become diseased through overuse, degeneration and trauma. The tendon can:
- Tear from the socket attachment.
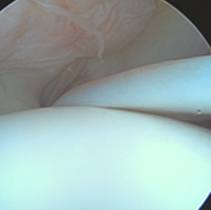
- Fray and split
- Enlarge so that it cannot fit in the tunnel as the arm is raised.
- Tear the tunnel ligament and jump out of the groove. This dislocation may damage the front rotator cuff tendon (subscapularis)

Eventually the tendon can rupture completely. This can cause bruising of the arm and biceps muscle “Pop-eye” deformity.
Long head of biceps pathology can occur in isolation or with other shoulder issues such as rotator cuff tears and arthritis.
Long head of biceps pathology can be assessed with ultrasound, MRI and at arthroscopy.
Treatment can vary depending on the specific pathology and associated conditions.
- Most long head of biceps ruptures in isolation can be managed non-operatively with minimal functional loss. If there is persistent cramping surgery may be required.
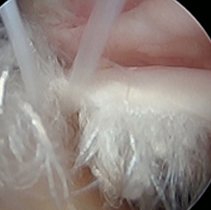
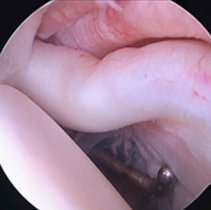
- If long head of biceps is noted on investigations or at surgery to be diseased, there is the option at surgery, to release the tendon from the joint (tenotomy) or release, excise the diseased segment and reattach the tendon (tenodesis).
Tenodesis restores muscle length, prevents cramping and the Pop-eye deformity. I perform a LHB tenodesis if the LHB is a possible cause of ongoing pain, stiffness or rotator cuff tendon damage. When released during arthroscopic surgery, I access the tendon through a small incision in the armpit front crease. The diseased portion is excised and the shortened tendon is reatttached to the upper humerus, using a whip suture and small titanium buckle. A small drill hole is made into the biceps groove and the buckle with tendon weave is introduced into the humeral canal. The button is flipped behind the front bone wall as an anchor.

The tendon takes approximately 3 months to grow into the bone and surrounding tissue, with lifting restricted to less than 2kg until 3months. Lifting can then be increased by 1 kg per week as tolerated. There also may be restrictions on lifting related to associated rotator cuff surgery.
Long head of biceps tenodesis is generally very safe. Uncommon risks specific to long head of biceps tenodesis include but are not limited to infection, frozen shoulder, nerve injury, re-rupture and the development of a chronic pain syndrome.




