Pectoralis Major Tendon Tear or Rupture
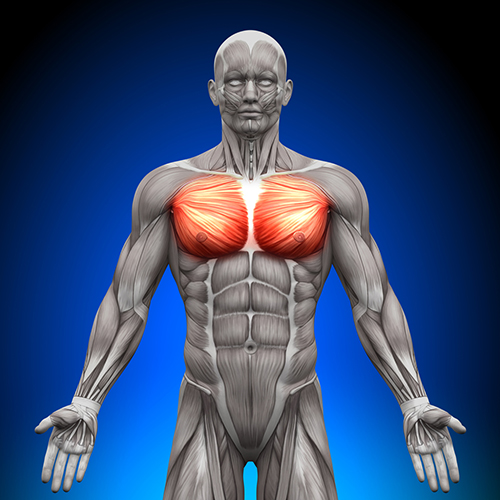
Anatomy: The pectorals major muscle is located on your chest under the breast. It has a broad attachment from the collarbone and upper 6 ribs. Its tendon inserts on the upper humeral shaft. The pectorals major muscle is a powerful shoulder internal rotator, adductor and forward flexor.
Mechanism: Rupture of the pectorals major tendon attachment has increased with greater participation in weightlifting, body building, wrestling and contact sports. Rupture occurs when the maximally contracted muscle can no longer hold the force, as occurs when the bar is descending in benchpress (eccentric contraction). In rugby it occurs when a player reaches to tackle in an abducted externally rotated (throwing ball) position. The use of anabolic steroids increases the risk of tendon rupture. The tear may involve all of the tendon (clavicular and costal heads) or more commonly part of the tendon (80% costal head only). The tendon may rupture off the bone or tear at the muscle tendon junction.
Clinical Features: At the time of injury, there may be a loud noise or tearing sensation. There is acute pain, swelling and deformity of the breast muscle and front of the armpit. Extensive bruising may develop down the inner biceps muscle and anterior chest wall. Weakness is noted with a push-up type action.

Diagnosis: The diagnosis can usually be made on history and clinical examination. The extent and location of the tear can be assessed with MRI (below).

Treatment: Will depend on individual factors such as activity level, percentage and location of tear and tolerance for residual weakness and cosmetic deformity.
Non-operative treatment involves sling immobilisation for comfort, analgesia and gradual restoration of function. This is best reserved for muscle tears, partial tears and in sedentary individuals.
Operative treatment involves reattaching the torn tendon to its origin on the upper humerus. This is performed through an incision in the front crease of the armpit. The tendon is located and secured using shoe lace type braided tapes. The tapes are loaded into a specially designed small titanium buckle that is inserted into small drill holes on the humerus. The buckle is flipped behind the cortical bone allowing the tapes to be sequentially tightened, holding the tendon on the original bony insertion site.

As with most tendon reattachment this is easier to perform early. Delayed presentations may still be able to be repaired but need to be individually assessed.
The risks specific to this surgery are relatively small but include infection (<1%), nerve injury, frozen shoulder and retear.
Results: "The available literature strongly supports the early operative treatment ofcomplete pectoralis major tendon ruptures in athletes with primary repair of the tendon to the bone. This generally yields good functional results, with a high amount of (athletes)regaining muscle power and return to sports, accompanied by fast recovery and a low complication rate, and therefore is the treatment of choice in this patient group."1
Without repair there is weakness, cosmetic deformity and a higher risk of residual pain. After pectorals major major rupture, bench press strength has been shown to be reduced by 75% compared with pre-injury. 2
Post-operative rehabilitation: The rehabilitation is based around the biological healing time for tendon healing to bone. It takes around 12 weeks for the tendon to throw fibres into the bone, like a tree throwing roots into the ground. Until 12 weeks, the pectorals major tendon attachment remains dependant on the suture tapes and these are not strong enough to take resistance.
0-6 weeks: sling immobilisation with passive shoulder elevation and external rotation.


6-12 weeks: active range of motion, minimal load or resistance, light activities of daily living. Emphasis on restoring a full range of motion.

12 weeks +: gradual increase in lifting, strength, resistance and endurance.


Avoid benchpress until tendon healing is complete and there has been adequate return of strength (minimum 6 months). Benchpress re-injury can be minimised by reduction in lifting weight, experienced spotter, avoiding fatigue and hyperextension. Hyperextension can be prevented by performing bench while laying on the ground.

- Jörn Kircher et al. (2010) Surgical and nonsurgical treatment of total rupture of the pectoralis major muscle in athletes: update and critical appraisal, Open Access Journal of Sports Medicine, 1:, 201-205
- Shah, Nasir H. FRCS et al. Pectoralis Major Rupture in Athletes: Footprint Technique and Results. Techniques in Shoulder and Elbow Surgery 11(1):p 4-7, March 2010.




